Myasthenia Gravis: Causes, Antibodies, Manifestation, Diagnosis, Treatment
Jun 5, 2023
Navigate Quickly
Introduction
Causes of Manifestation
Antibodies
Prevalence
Manifestations
Diplopia
Diagnosis
Treatment
Treatment for Neonatal Transient Myasthenia Gravis
Lambert Eaton Syndrome
Clinical Features
Treatment
Neurasthenia
Botulism

The skeletal muscles, which our body utilizes to move, become weak due to the neuromuscular condition known as myasthenia gravis. Myasthenia Gravis develops when there is a breakdown in nerve-muscle connection. Myasthenia gravis is the most prevalent primary condition of neuromuscular transmission, according to the Myasthenia Gravis Foundation of America.
Scale up your NEET PG preparation with this blog on important topics for microbiology and experience the best NEET-PG coaching available online.

Introduction
It is a type of two hypersensitivity reactions. It's an autoimmune disorder which will be having a waxing and waning course. It will have exacerbations especially in pregnancy and infection and it could be worsening to a level that the person might require ventilatory support. That's called a Myasthenic crisis. It is also mentioned as type V hypersensitivity reaction, in some books. In myasthenia gravis the basic problem is the receptors for acetylcholine are the ones which are affected, It's a supposed junctional defect. Acetylcholine will act on its receptor having a total of five subunits:
- Alpha
- Beta
- Gamma
- Delta
- Epsilon
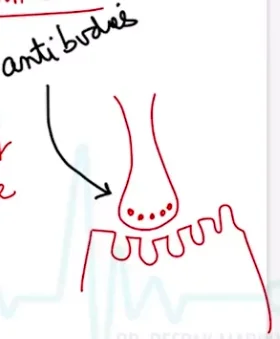
Alpha subunit is of concern because when it is activated, the sodium influx would be occurring subsequently causing a depolarization. There will be firing of the neuromuscular endplate, which allows the muscles to contract. The anti AchR antibody includes the following functions:
- It will cause blockage or blockade of the receptor. Blockade means it will mainly affect the alpha subunit, which means the contraction of muscles will also significantly reduce. This is called myasthenic fatigue.
- There would be an increase in the turnover of the receptors as well.The time for the acetylcholine to activate the receptor is reduced.
- In this the patient has physical damage as the antibody causes damage to the postsynaptic muscle membrane.
- Antibody affects the receptors and causes damage to the muscle membrane.
- The fourth problem in this condition is called presynaptic random. It is said that the pre-junctional site is causing release of acetylcholine, But it does not activate the receptors. The presynaptic release of acetylcholine, can be marginally affected. This ultimately contributes to the disease process.
The common parameters is that due to all these effects, the efficiency of neuromuscular transmission is affected significantly and it reduces the ability of the muscle to perform.

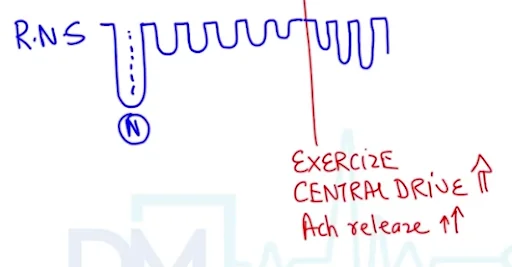
The above image shows a Repetitive Nerve Stimulation test in which you stimulate a nerve at a lower frequency than at a high frequency. When you stimulate the muscles as they keep on performing, their performance reduces. Usually the performance reduction is less than 10%. A substantial reduction in the performance of the muscle is seen. This is because the nerve is being continuously stimulated. The reason for this is that the acetylcholine is not being able to activate its receptors properly due to various reasons. The technical term is Decremental Response.
Causes of Manifestation
Clinical studies have shown that 75% of patients of Myasthenia Gravis are having a thymus abnormality (65% are having a thymic hyperplasia and 10% are having a thymoma). Thymoma is a benign tumor,which can spread locally and it can press on the recurrent laryngeal nerve.
The thymus is having the cells that are called myoid cells as antigens. On the surface of these myoid cells, there is an alloantigen. This is the antigen against which antibodies are formed and the chemical structure of this antigen resembles the acetylcholine receptor. When target receptors are affected, then the functioning of muscles will be affected. Antibodies present are T cell dependent and IgG class which can cross the placenta. If a mother or a young lady has autoimmune disease, she can transfer this antibody to her baby, and congenital myasthenia gravis or neonatal Myasthenia Gravis will be a presentation in this case.

Antibodies
- Anti acetylcholine receptor antibody (in about 85% patients)- This will block the receptors of acetylcholine which affect the alpha channel. So acetylcholine won’t be able to go in.
- Anti Musk antibody ( in about 10% patients)- The full form is muscle specific kinase antibodies. It is Mostly in those patients who are AchR negative.
- Anti LRP4 antibody- The full form here is low density lipoproteins related protein 4 antibody.
- Anti Netrin-1 receptor antibody
- Anti Caspr-2
- Anti striated muscle antibody
Prevalence
It has a figure of 200 cases for every 100,000 people in Western populations. It is common in young women or in men after 50 to 60 years of age. The disease can be showing an exacerbation it will be having a waxing and a waning course. The exacerbations can be triggered by infection, or by pregnancy. The young female might be fighting for her life at the time of pregnancy when she goes into a myasthenic crisis. During which, there will be a diaphragmatic paralysis developing in a patient.
Manifestations
- Ptosis- It is the earliest manifestation present.

This picture shows a young lady who's suffering from Myasthenia gravis. She has involuntarily elevated her eyelids to keep her eyes open when she was asked for medical photography. Initially, most patients having Myasthenia Gravis don't realize that they're having ptosis. Persons having ptosis use the forehead muscles to elevate the upper eyelids.
Diplopia

The cornea and the upper two millimeters on the cornea is always covered by the upper eyelid. In patients of Myasthenia Gravis when they wake up in the morning they will not have any ptosis but suppose the patient is watching television news or they are fiddling around with a smartphone, then there will definitely be stress on the eye muscles and that will trigger a ptosis. And when we examine the patient, we will notice that this Ptosis is never symmetrical. It will always be the asymmetrical ptosis developing in a patient.
If this patient has not watched television, then the patient will say that in the morning they are feeling fine but by evening the patient is not sleepy, but still her colleagues are asking her why she looks so sleepy. And if this person is working on a computer in the office, she will have to involuntarily use her forehead muscles to elevate her eyelids to type on the computer. As there is asymmetrical ptosis that explains why there will be a double vision developing in the patient. So in these patients we will request this person to simply do an upward gaze for as little as 30 seconds and there will be a development of symptoms of ptosis and diplopia in the patient. Some patients might be having only the extra ocular muscle weakness as a presentation for the whole of their life . If the symptoms of extra ocular muscle weakness persist for more than three years then the term that is used to describe is called ocular myasthenia gravis. In this case, we should do a CT or an MRI to rule out any CNS cause that can also contribute to ptosis. Here, the problem is not any mass effect of any tumor or aneurysm going in the brain but it is a neuromuscular function at the junction not occurring properly. Now, we have asked this lady to smile which in this case, would be a snarling appearance coming up. So patients of Myasthenia Gravis are set to have Snarling faces which is a feature of myasthenia gravis. They may not be visible initially.
- Chewing Muscle Weakness-
This is based on the fact that when this person is eating non veg food, it is taking longer for the patient to finish the meal . So, pharyngeal muscles, tongue muscles, cannot function normally. So the ability to eat fast and the ability to swallow food fast will not be present in these patients. Chewing muscle is a more prominent muscle weakness which is exaggerated on eating non vegetarian foods especially meat or mutton etc..
- Nasal Twang-
If we talk continuously we still have the same voice, pitch. But in these patients because of the weakness of the pharynx, muscles of the throat, there can be development of nasal twang. Especially the weakness of the soft palate.
- Nasal Regurgitation-
There can be nasal regurgitation of fluids. When the person drinks water, coke, it might come out of the nose.
- Aspiration Risk-
Here the aspiration risk will be so high that we will have to admit the patient to the Intensive Care Unit and manage the patient conservatively.
- Dysphagia-
With Dysphagia, it might seem that the esophagus is involved. But esophagus is smooth muscle and this is a disease of the skeletal muscle. Because the tongue cannot perform like a normal person, we are using the word oropharyngeal dysphagia.
- Dysarthria
In some patients, even muscles related to vocal cords will be affected. There are two reasons why the person is not able to speak properly. One is the Nasal Twang of the voice and The second is dysarthria related to muscles with the vocal cord. We can go on speaking hours without any change in the pitch and quality of the voice. But in these patients, the unclear speech will start developing after continuous speaking for two to three minutes.
- DTR Preserved
The deep tendon reflexes in these patients are preserved. The muscle weakness is prominent in these patients; it increases with activity of the same muscle. There is a diurnal variation of features in these patients. But in spite of all this motor weakness, the reflexes in these patients are preserved unlike Lambert Eaton syndrome. The DTR would be normal in these patients. Sensory function is not affected in these patients so sensation in the throat is preserved. There's no problem with the gag reflex per se.
- Proximal Muscle Weakness-
In this condition there is arm and leg weakness in Myasthenia Gravis. If we ask this person to spread out arms and keep arms abductors up, then we will notice that even shoulder muscle fatigue will start developing and they will be drooping in the arms of the patient. So, muscles of the hip joint muscles of the shoulder joint can be involved but as a late manifestation in the disease. In Lambert Eaton syndrome, the primary complaint will be proximal muscle weakness. So, suppose there is a female, she has long hair. She says when she comb her hair, she feels as if the comb has become heavy. So when she used to do this brushing activity or combing the hair activity that deltoid weakness used to manifest in the person.
Diagnosis
- Anti AchR Antibody- The screening test will be answered by the antibody which is an anti acetylcholine receptor blocking antibody. This is positive in 85% of the cases. If this is positive, the probability of diagnosis has increased, but this antibody can be negative as well.
- Anti Musk antibody- This is known as a muscle specific kinase antibody.
- Anti LRP 4
- S.F.EMG- SFEMG is single fiber electromyography. The findings in this case would be referred to as a jitter and blocking which means that the amplitude of contraction will not be substantial as it should be as a normal muscles performance. It is expensive and may not be available in most government hospitals.The term Confirmatory test has been used for this. Electro diagnostic tests are always to be given preference over anti cholinesterase test or Tensilon test.
- RNS- The neurology department might tell that they are doing the tests by the name of repetitive nerve stimulation tests. In this, we just need to purchase some electrodes and you should obviously have a setup where you can record the discharges of stimulation of the muscles when we stimulate a particular nerve. It is relatively cheaper and it will show a classical decremental response.
- Anticholinesterase Test / Tensilon Test- The first step in the tensilon test is to ask the patient for a sustained upward gaze that will trigger Ptosis in the patient; it would be asymmetrical bilateral ptosis. We have secured an IV line by the time the ptosis will start occurring in the patient. When the The IV line is in place, the nurse will give a syringe that contains 10 milligram of edrophonium.
This molecule is a short acting anti anticholinesterase agent. If you will give this injection intravenously the onset of action will be after 30 seconds and the maximum duration of this drug is five minutes. We do not push 10 milligrams right away because it can trigger a cholinergic crisis. So first we will give two milligrams which will inhibit the degradation of acetylcholine.
As we are inhibiting the degradation of acetylcholine, it will be able to act on the receptor for longer duration. Most of the time when you give two milligram of edrophonium, there will be a marked improvement in the patient.If there is no improvement, then we can give the remaining eight milligram of edrophonium to the patient and wait for a clinical response. We will look at the ptosis component or we can ask the patient to separate the arms before and after the performance of the test and see how long he can hold the arms in abduction position. So, we have three things :
- First Ptosis will become lesser then will become absent and then will reappear because the effect of the injection will go away.
- Cholinergic crisis will be identified when the patient will develop sludge symptoms that would be hyper salivation because of excessive acetylcholine.
- There have been instances when patients have become really very sick like during the performance of the test the patient literally aspirator saliva had to be admitted into ICU.
It is on the backseat or it is not given in the front primarily because of hyper Salivation, hyper lacrimation. There is frequent urination, diarrhea, gastrointestinal complaints, and miosis in patients. During the performance of this test, if we are having a volunteer crisis, Atropine has to be given to the patient.
- Ice Pack Test-

(Ice Pack test- alternative of Tensilon Test)
There is a man having asymmetrical Ptosis. Now we have taken some ice , rolled it in a glove or maybe a commercialized pack which comes with vaccines, etc. And we put it on the patient and we notice that after applying the ice pack for 3-5 minutes, the Ptosis of the patient has substantially reduced.
The application of ice is contributing to reduction in the symptoms. Acetylcholinesterase is very sensitive to temperature. If we decrease the temperature, then the activity of acetylcholinesterase enzymes tends to reduce. So there is decrease in turnover of receptors and acetylcholinesterase is lesser, acetylcholine will not be broken down and therefore there will be a better action available. The test of the ice pack has a sensitivity equal to that of the tensilon test.
- CT/ MRI Head- It helps to rule out causes like arteriovenous malformation or any space occupying lesion contributing to third nerve Palsy or ptosis occurring in a patient. This is a baseline test that is mandatory in all cases of ocular myasthenia gravis.
- CT Chest- It is done in the patient because we want to pick up Mass Effects of thymoma. We also want to demonstrate whether there is a thymic hyperplasia in a patient. Thymectomy is done in all cases because even if it is a patient who will require steroids, the dosage of steroids is reduced. If we are having lesser requirements of steroids, then the side effects of steroid toxicity are substantially reduced. CT chest is to be done to rule out the thymus abnormalities in the patient.
- Hashimoto / Grave / SLE / RA- In the workup of these patients, We need to do an antinuclear antibody. We will do a RA factor in the patient. And a baseline TSH can be done in the patient. Because in Hashimoto, if the person has reached a hypothyroid state, then the values of TSH will be high and in Graves disease, the TSH values will be literally undetectable.So, TSH anti nuclear antibody and RA factor is done to check for Co- existent autoimmune diseases which could be present in this particular condition.
- PFT- One pulmonary function testing is done in all patients because we need to plan a thymectomy for these patients. We would look at the lung reserve of the patient. If he's an obese person because possibly the person who has Myasthenia Gravis might have been on steroids for a long duration. So the obesity component might have developed in a patient. We will check this before we plan a surgery for a patient. Then because we give steroids for immunosuppression in all patients of Myasthenia gravis, immunosuppressive drugs like prednisolone have to be given. If tuberculosis is present in a patient or diabetes is present in this patient co-existent, then they will worsen. Steroids will worsen tuberculosis or diabetes mellitus by increasing the blood sugar values.
- HbA1C, TST- The glycosylated hemoglobin values and a baseline test for TB like tuberculin skin test will be done.So diabetes mellitus and tuberculosis should be ruled out by the investigation part before initiation of immunosuppressive therapy is done for these patients.
Treatment
- There is a usage of pyridostigmine. In pediatric cases, Neostigmine is given to the patient, but in adult cases it is the Pyridostigmine which is the best drug to limit the symptoms. The onset of this medicine is after 15 minutes and the total duration of action is approximately four hours. So repeated doses of Pyridostigmine have to be given to these patients for causing symptomatic relief.
- Anti MUSK- Patients who are having these anti MUSK antibodies present may not show a good response to this drug. In generalized Myasthenia Gravis the response is going to be much much better. We have to keep a watch for persons who are anti musk antibody positive when they should follow up with you regularly because worsening has been documented with Pyridostigmine but it is a preferred drug to be used or DOC from pharmacological perspective is obviously Pyridostigmine and not neostigmine.
- Thymectomy- Thymectomy is the treatment of choice for generalized Myasthenia Gravis. There are two aspects why thymectomy is used: One, it is always to be done for resection of thymoma because it can expand locally. It's a benign tumor, but it can expand locally and cause a Mass Effect. Secondly, they haven't documented the fact that even if a person is not having a thymoma, suppose is having a thymic hyperplasia, it is advantageous to remove the thymic hyperplasia because the subsequent requirement of steroids that you prescribe for these patients in the long run significantly reduces. Before doing a thymectomy a pulmonary function testing must be done thoroughly. The anaesthesiologist should be clear with respect to the lung function of the patient because we don't want any postoperative complications because anything you know, surgery can also trigger a myasthenic crisis in the patient. So the anaesthesiologist has to be good at ventilation both intra and postoperatively for these patients, it might take a while for these patients to come out of anesthesia also. So therefore, the anaesthesiologist has to be the one who has previously handled cases of Myasthenia Gravis because interrupt complications and post op complications in these patients will be more especially with ventilatory drive being limited in these patients secondary to diaphragmatic involvement. Second is the decrease in the requirement of immunosuppressive drugs because long term intake of steroids can cause Cushing's Syndrome, visual defects, cataract innovation myopathy in a patient. Our objective in generalized myasthenia gravis is mainly to convince the patient to sign up for thymectomy as early as possible.
- In ocular myasthenia gravis, we first give Pyridostigmine and if it's a poor response, then straight away go for immunosuppression. We do not recommend thymectomy in ocular myasthenia gravis. Studies have shown that for ocular myasthenia gravis, the first line drug is pyridostigmine obviously for symptomatic relief.Though if a person is anti muscle specific antibody positive there might even be worsening, so a watch out for the same has to be kept. If a person is having a poor response to administration then we have to start these patients on immunosuppressive molecules like steroids and azathioprine.
- In generalized Thymectomy -first give pyridostigmine and you will get a substantially good response in the patient.
- Now educate the patient regarding the benefits of thymectomy. Because we have to start the person on immunosuppressive medication as it's an autoimmune disorder.
- If the FVC of the patient is good, and the consent of the patient is there, then a thymectomy can be performed in the patient.
- Post thymectomy, in these patients, we will still be giving steroids but the dosage of steroids that would be required in this particular case will be minimalistic.
- The requirement of immunosuppressive therapy after thymectomy is substantially reduced.
- In Myasthenic crisis patients, we will use plasmapheresis for these patients to get rid of the dangerous antibodies.infection and pregnancy are triggering factors.If facilities for plasmapheresis are not available. It is intravenous immunoglobulin. The first to be done in the Myasthenia crisis is obviously elective intubation and ventilation of the patient. We will have to maybe put the patient on assisted controlled mechanical ventilation because the PCO2 to the patient is beginning to rise in co2 in the patient is significantly low. So, the crisis has to be managed on a war footing.
Treatment for Neonatal Transient Myasthenia Gravis
Neonatal Myasthenia Gravis means that the mother of this child was having Myasthenia Gravis and at the time of delivery and before delivery, she has transferred the antibodies to a child.
- The antibodies that are found in this condition are immunoglobulin G class which can very easily cross the placenta.
- Because of the transplacental spread of this antibody, the neonate will also suffer from a possible difficulty in establishing respiration.
- Therefore, a trained neurologist or a pediatrician should be available to take care of the airway of the child.
- Breastfeeding will still be a challenge because every time she will breastfeed this baby, there might be regurgitation of milk, they might be choking episodes
- When she asks what is to be done, we are prescribing some drops (neostigmine) for the child which have to be given regularly to your child every three to four hours. She agrees but asks the time.
- If she breastfeeds the child without these drops. The child can aspirate and die.
- Antibody has not been produced by the immune system of the baby the antibody has been produced or has been transmitted from body of the mother to the baby the baby has acquired this antibody from the mother.
- Every antibody is a half life IgG usually gets destroyed by 23 days.
- So we would tell her that after four weeks of life because this antibody will be destroyed by the immune system of your baby, he will not require any medication.
- After four weeks, this child will not suffer from any problems because the antibodies will be cleared by the immune system of the child.
- This explains the fact that neonatal transient Myasthenia Gravis has a good prognosis.
- So the drug of choice for neonatal transient Myasthenia Gravis is neostigmine for our early for the first one month of life, and then it is goodbye to the disease forever.
Lambert Eaton Syndrome
When it comes to a male patient the association is with aggressive lung cancer that is small cell cancer of the lung. So this can be a paraneoplastic manifestation related to lung cancer. In this, the problem is that the production of acetylcholine is lesser. This is a pre synaptic disease whereas Myasthenia Gravis is a postsynaptic, post junctional disease where the receptors of acetylcholine are defective. This is a presynaptic disease in which the release of acetylcholine is compromised.
Let us assume that this is where the acetylcholine will be released and we have the receptors available.There is production of antibodies when muscle is stimulated. The antibodies which are present here, they go and attack the neuromuscular junction, but they do not attack the receptors. Now the antibodies will act on the pre junctional site and reduce the acetylcholine release because of which we are calling it a pre junctional defect. Therefore, due to less stimulation, the contraction of muscles and this condition will also be relatively less.
Clinical Features
- Proximal Muscle Weakness- Not eye or ocular muscle involvement and chewing muscle involvement.
- Subsequently the feature will be ptosis, diplopia Chewing muscle weakness might be there. So it might begin by saying a female. The incidence of lung cancer is the main component mainly seen with male patients or Lambert Eaton syndrome. In females they may not be associated with lung cancer so that way the prognosis will be better in females.
- DTR- Deep tendon reflexes are preserved in patients with myasthenia gravis, but here the deep tendon reflexes in these patients will be substantially reduced. So, reflexes can be one point of differentiation.
- Autonomic Features- Second differentiation can be autonomic associations in these patients. It can include dry mouth, or male patients having erectile dysfunction.
- RNS- Repetitive nerve stimulation response. It is the main differential point. The amplitude of contraction of a normal person versus Lambert Eaton syndrome, we will always be having very poor contractions or weak contractions occurring in the patient.
You can imagine this to be normal amplitude or contraction for any one. So, nerve stimulation versus Lambert Eaton where the contraction is really poor. Because this contraction is poor, we will ask the patient to do some stretching exercises, such as move your arms or do some squats if you can. When the person exercises what happens is that the central drive in the body will increase with increased acetylcholine release at the neuromuscular junction. So if we test the person post exercise, we will notice that the amplitude or contraction will be relatively better. It is not normal but we can notice there is a substantial increase in the amplitude of contraction.This is what is called an incremental response.
The name of the antibodies involved here is antibody P/Q antibody and this is acting voltage sensitive calcium channels which help in release of acetylcholine at the neuromuscular junction.
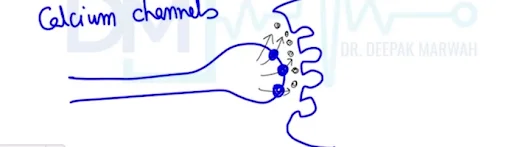
If this is the representation of the terminal end of any nerve, we have calcium channels which are present at the top; these are the receptors for acetylcholine. The calcium channels are the one through which quanta of acetylcholine (That is why when the calcium channels will open, then acetylcholine release will be occurring.) So these are the molecules of acetylcholine, they are lesser in patients of Lambert Eaton syndrome, and the receptors are performing fine. If we upgrade the amount of acetylcholine at the NMJ, then the performance of these patients will increase whereas in Lambert Eaton in comparison to Myasthenia gravis will have blocked receptors.
Treatment
The drug of choice for this condition would be 3,4 diaminopyridine. This will increase the amount of acetylcholine at the neuromuscular junction. This drug basically acts on potassium channels. Along with this we can add pyridostigmine. The advantage of Pyridostigmine treatment will be that it will inhibit the degradation of the release acetylcholine.
Neurasthenia
The symptoms that are described by a neurasthenia patient might be the same as that of myasthenia gravis. So, it will be easy for fatigue to occur in a patient. But there is no organic cause in this case. Symptoms will be identical to Myasthenia fatigue. But there is no organic basis in this case and the testing of the patient will be normal. And the history of this patient will keep on changing like sometimes a patient will say he is weak in the morning or afternoon or evening. And we will find discrepancies every time. Like there is a plain lazy person. He or she is having symptoms that might look like Myasthenia gravis, but then there is no organic basis beyond development of the disease.
Botulism
Here, there was a home delivery and the grandmother had given honey to the baby.
This would be a disaster because if the quality of the honey is bad, honey was given and the spores of botulinum toxin will germinate in the GI tract and will produce the toxin. Therefore, the patient will develop paralysis that will be a descending paralysis. Most patients of Botulism would be newborn babies who would be having bulbar palsy. The bulbar Palsy would explain the aspiration of milk, inability to feed or nasal regurgitation of fields in this child and they can also be diaphragmatic paralysis which can be life threatening. The main treatment for botulism would be to give antitoxin for this patient. This is an unfortunate complication and lots of time even without a diagnosis the child might actually die.This is also a pre junctional defect or a pre synaptic defect, so the amount of acetylcholine the toxin acts on the neuromuscular junction, and it reduces the amount of acetylcholine release at the neuromuscular junction. ;So, the common thing between Lambert Eaton syndrome or botulism is only the decrease of acetylcholine release, but the age of presentation and the Allied features are grossly different.
MG vs LEMS
| Myasthenia Gravis | Lambert Eaton Myasthenic Syndrome |
| Mainly Associated with Thymus Abnormalities | Associated with small cell lung cancer, especially with male patients |
| Acetylcholine release is completely normal. Problem is with the receptor known as Post Junctional Defect. | Acetylcholine release is less. Receptors are however normal. |
| Multiple antibodies but main are: AchR antibody Anti Musk Anti LRP4 | Antibody: Anti P /Q (calcium channels) |
| Might be having Ptosis, extra ocular Muscle weakness, Diplopia, Chewing muscle weakness | Might be having Ptosis, extra ocular Muscle weakness, Diplopia, Chewing muscle weakness |
| It begins by saying a female but she will straightaway start from ptosis diplopia he will not talk about proximal muscle weakness. | Features Shoulder Girdle weakness, Proximal Muscle weakness |
- Anti acetylcholine receptor blocking antibody if it is negative, that does not rule out the possibility that disease or disease could still be present in a patient, it's for screening.
- But to confirm you always need to go in for not repetitive nerve stimulation. It is single fiber electromyography which is the confirmatory test for diagnosis of this patient.
To scale up your NEET PG preparation with the best-in-class video lectures, QBank, Mock Tests and more, download the PrepLadder App!
Download PrepLadder's NEET PG preparation app for Android
Download PrepLadder's NEET PG preparation app for iOS
PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Top searching words
The most popular search terms used by aspirants
- NEET PG study tips
- NEET PG Microbiology